- News
Department of Thoracic Surgery Applied Single Small Incision Thoracoscopy to Removed A Large Mass for a 7-year-old Girl
Link of the Original Article:
https://mp.weixin.qq.com/s/TStKxX3jAhd6bOopxRisrQ
A 7-year-old girl came to the clinic of Dr.Huang Wei, who is thoracic specialist and staff surgeon, because of recurrent coughing for 4 months. Her plain scan CT showed a large mass in the lower lobe of the left lung with maximal diameter about 6-7cm.
The girl had just started her life in elementary school with dream of bright future. The finding of large mass in her lung made the whole family so worrisome that her parents took her to some thoracic specialists, who suggested open surgery for treatment. Open surgery with a big incision is really not only a trauma for such a young girl physically, but also for her parents mentally. So when they anxiously asked , "Could it be cured safely in a less traumatic way?”. The reply they got was “of course, could use minimally invasive way”.
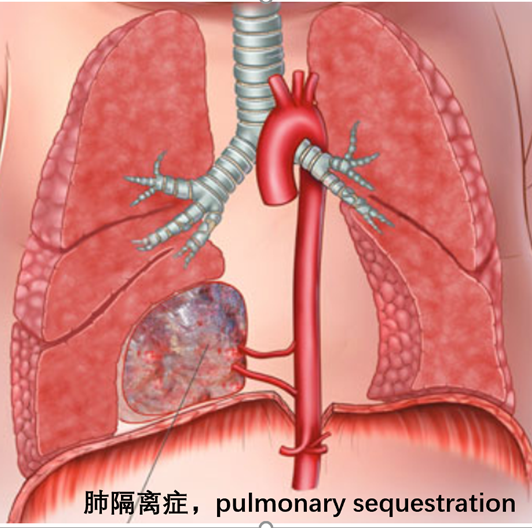
For a pulmonary surgery, it’s very important to differentiate lung masses. Keep in mind: not all lung masses for that anti-infection treatment is ineffective are diagnosed as lung cancer. Pulmonary sequestration is one of the diagnoses that need to be differentiated regarding the children with recurrent lower lobe pneumonia.
Pulmonary sequestration is a common congenital malformation of the lung. The lungs of normal people mainly receive blood from the pulmonary artery. Venous blood with low oxygen content is ejected from the right ventricle, reaches the pulmonary capillaries through the pulmonary artery and its branches for gas exchange, and then returns to the left atrium through the pulmonary vein. This is called pulmonary circulation. It is the key link for oxygen diffusion into the blood and carbon dioxide escape from the blood.
Some lung tissues of patients with pulmonary sequestration mainly receive blood from systemic circulation arteries due to congenital development abnormalities. There are problems in the communication between these abnormal lung tissues and normal bronchial trees, and as well as in gas exchange of pulmonary capillaries. This part of abnormal lung tissue is completely different from other functional normal lung tissues. It seems to be "isolated " from normal airway ventilation and circulation, as its’ name implies.
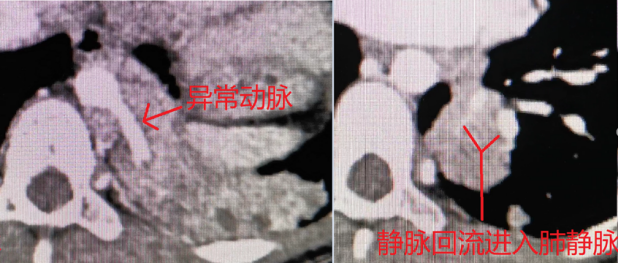
The contrast CT was performed and showed a large lesion in the left lower lobe which lacked communication with the normal bronchial tree and had abnormal blood supply of thoracic aorta. The vein of the lesion returned into the pulmonary vein. Intralobar pulmonary sequestration was considered in the clinical setting.
In "intralobar type" of pulmonary sequestration, abnormal lung tissue exists in the lung lobe and is wrapped by the same pleura as the normal lung. The clinical features were recurrent pulmonary infection with coughing, expectoration, hemoptysis and low fever. Intralobar pulmonary sequestration should be considered in patients with recurrent pneumonia in lower lobe. The abnormal blood supply artery usually comes from the thoracic aorta, abdominal aorta or intercostal artery and the vein returns to the pulmonary vein, rarely to other adjacent veins. There are more cases of Intralobar pulmonary sequestration on left side than right side, most commonlly in the basal segment S7 and the posterior basal segment S10 of the lower lobe.

In "extralobar" pulmonary sequestration, the abnormal lung tissue has its own pleura and is separated from normal lung lobes. The clinical manifestations are relatively elusive and a majority of patients are asymptomatic, while some patients may have symptoms of infection or respiratory dyspnea caused by compression of large mass. The abnormal blood supply artery mainly comes from thoracic aorta or abdominal aorta, but the vein of it often returns to the azygos vein, semi azygos vein or portal vein system, and only occasionally to the pulmonary vein.
The operation of Uniportal VATS for this little girl was scheduled soon after careful and comprehensive preoperative evaluation. We placed the thoracoscopy through a small single incision about 3cm in the fifth intercostal space. First, we finded an area of consolidation in the lower lobe of left lung. Then we opened the posterior mediastinal pleura and identified the abnormal blood supply artery from the aorta above the diaphragm, and dissected it under the endoscope with vascular stapler. This step is the key of such kind of operation for pulmonary sequestration. It is worthy to mention that the wall of the abnormal blood supply artery is thin and fragile and high blood pressure from systemic circulation, all of which could cause massive bleeding by accidental injury. So in such case, it is necessary to keep careful and gentle when managing the abnormal supply artery. It is strongly recommended that the safest strategy is to find abnormal artery and dissect it in a reliably secure way at first. The remaining steps are basically the same as the procedure lobectomy by single hole thoracoscopy (uniport VATS).
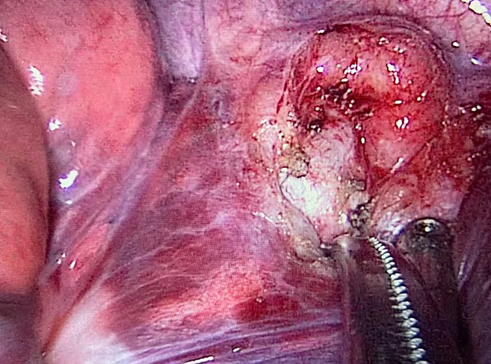
Consolidated lung lobe
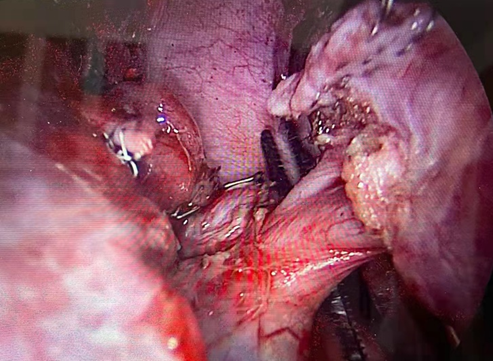
Dissection of abnormal artery
In the intralobar type of pulmonary sequestration, the isolated diseased lung and normal lung tissue are covered by the same layer of parietal pleura, and the boundary between them is not clear. If only the abnormal lung tissue is removed during the operation, the surgical wound on the lung is often too large, which could lead to some complications such as serious air leakage ,infection and so on. The classic surgical method is lobectomy, that is, to remove the whole lung lobe with pulmonary sequestration. Sublobar lobectomy is only attempted for a small lesion without concurrent infection. The surgical method of extralobar pulmonary sequestration is relatively clear and easy, that is resection of the isolated lesion.

In the past, open surgery (thoracotomy) was often used for children's lobectomy. In recent years, with the development of endoscopic technology and anesthesia, more than 90% of the operations in the Department of Thoracic Surgery were performed by single small incision thoracoscopy (uniport VATS). A very small incision about 3cm was made in the chest wall, which not only reduces the chest wall trauma and pain, but also makes the incision more beautiful. The single incision thoracoscopy team led by Dr. Fan Jiang ,director of the Department, and Dr. Wu Liang and Dr. Huang Wei has broadcasted lung surgery for many times. The operation is skill-required and meticulous, and is widely preferred by domestic and foreign surgeons and also patients.
The little girl's recovery was very smooth. On the fourth day after the operation, the drainage tube was removed and she was discharged from the hospital. The symptoms of repeated pneumonia also disappeared. The family finally got relieved.

This is a classic case of pulmonary sequestration with recurrent pneumonia. In addition, a small number of children with pulmonary sequestration can be asymptomatic for a long time until they are found incidentally in the physical examination during adulthood. About half of the patients with extralobar pulmonary sequestration are complicated with other malformations, of which congenital diaphragmatic hernia is the most common and can be treated together during the operation. There are also some children with extralobar pulmonary sequestration who have more severe feeding difficulties, dyspnea and other symptoms, and need timely diagnosis and surgery. Extralobar pulmonary sequestration can also cause congestive heart failure. Because its veins flow back to systemic circulation veins, it is equivalent to a "short circuit" between the aorta and the large veins, wasting the output work of the heart. Such children often have symptoms in the first few months after birth. In serious cases, intravascular interventional embolization of the blood supply artery can be considered first, and surgery can be performed after the condition is stable.
Reference material:
1.Corbett HJ, Humphrey GM. Pulmonarysequestration. Paediatr Respir Rev. 2004; 5(1):59-68.
2.Hendrik C. Dienemann,Hans Hoffmann,FrankC. Detterbeck,Chest Surgery,2015.
3. Jingzhe Zhang, Pediatric Surgery (2nd Edition), edited by Xin Ni, 2020
4. Physiology (9th Edition), edited by Tinghuai Wang, 2018